
Caitlin Stowe MPH, CPH, CIC: “There’s still a lot we don’t know about SARS-CoV-2 and the direct mechanisms of transmission…. It can be aerosolized. However, there is evidence of indirect transmission from surfaces to people.”
Caitlin Stowe MPH, CPH, CIC: “There’s still a lot we don’t know about SARS-CoV-2 and the direct mechanisms of transmission…. It can be aerosolized. However, there is evidence of indirect transmission from surfaces to people.”

Kevin Kavanagh, MD: “If we keep spreading this virus around, it’s going to slowly devastate both our population and our economy.”

Mary Jean Ricci MSN, RNBC: “[Infection preventionists] really need to think about how we’re getting people from the assessment area to the vaccination area to the evaluation area in a unidirectional flow so that we don’t have the spread of the virus at the time of inoculation.”

Sharon Ward-Fore, MS, MT(ASCP), CIC: “Infection preventionists need to remind people to be vigilant both in health care and outside of health care. Because we’re not done with this yet. We have a long way to go before we’re fully protected.”
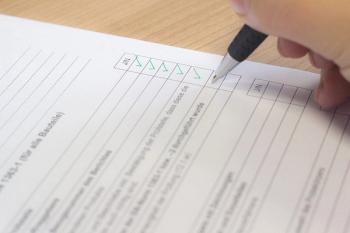
Too often the tracking of the use and disinfection is done with pen and paper. That's what leads to problems, says Michael Cousin.

Anthony Harris, MD, MBA, MPH: “There are a number of ways that [infection preventionists] are going to continue to be on the frontlines helping us fully understand the impact of COVID-19 and get to the other side of it.”
Devin Jopp, EdD, MS: “I think from sports teams to hospitality to construction sites, to many, many more, the infection prevention field will absolutely be bulging.”

Linda Spaulding RN, BC, CIC, CHEC, CHOP: “There’s not enough literature out there yet to say that once you get the vaccine, you won’t get COVID again, and the literature that is out there says that once you get the vaccine, even if you don’t get COVID again, you can still be an asymptomatic carrier.”
Cedric Steiner: “But the nursing home…. One could make an argument that [infection control is] more important there in some ways, because you have those residents in smaller spaces."

Linda Spaulding RN, BC, CIC, CHEC, CHOP: “Infection preventionists need to learn how to clean an endoscope, or at least observe the cleaning…. Infection preventionists need to make rounds, they need to talk to the person processing.”

Kevin Kavanagh, MD: “One of the things that’s really frustrated me with this epidemic and pandemic is that people are totally focused on dying…. But in actuality, the disabilities are much, much more concerning because that is even affecting the young people.”
Maureen Vowles: “I think that the relationship between infection preventionists and public health is key to the success of preventing CRAB and other multi-drug resistant organisms.”

Kristy Warren: “We need to do everything we can to help protect our providers when performing these aerosol generating procedures. And subsequently those providers that enter the room or exit the room after these procedures have occurred.”

Ravi Starzl, PhD: “If you’re constantly focused on trying to escalate the war of destruction, I think that the bacteria will always win that war. They just have too many countermeasures available to them and our rate of developing new antibiotics is far slower than their rate of developing countermeasures.”

Bruce Y. Lee, MD, MBA: “We have to remember that infection control and prevention is not just dealing with the pathogen itself but dealing with the consequences and the downstream effects of what happens when you are dealing with the pathogen.”

Sharon Ward-Fore, MS, MT(ASCP), CIC: “If it were my institution, I would make sure that infection preventionists are educated on everything they need to know about the COVID vaccine, as well as the flu vaccine side effects.”
Rebecca Leach: “I think the biggest thing is just having support, whoever it is. If it’s a fellow infection preventionist…. It really is that emotional support of being able to talk to each other about your experiences and really process your feelings.”

Kevin Kavanagh, MD: “I would tell the Supreme Court that it’s very important that all high-risk venues are treated equally, but the remedy isn’t opening up one high-risk venue, the remedy should be closing down all high-risk venues.”

Susan E. Campbell, PhD, CIC, offers advice to infection preventionists and other healthcare professionals who’ll be working Thanksgiving on how to safely eat their holiday meal together.

Kevin Kavanagh, MD: “We can’t just bury our heads in the sand and bleed through healthcare staff and bleed through PPE, thinking that this is not going to be something that’s going to cause severe problems in these individuals, or that it’s going to magically disappear next week."

W. Frank Peacock, MD, FACEP, FACC, FESC: “When I intubate somebody, I need to know where the tube is, and I need to know now—like within 10 seconds. You can’t tell with anything else. Nothing is as fast as the stethoscope. I can get an X-ray, but I’ve got to wait for the X-ray while you hold your breath.”

Caitlin Stowe, CIC, MPH, CPHQ, VA-VC: “The cool thing about being an infection preventionists is that I call myself the jack of all trades, but the master of really none. Because you really have to know a little bit about everything.”

Linda K. Groah, MSN, RN, CNOR, NEA-BC, FAAN: “Historically, we have not always had the best relationship. There’s been some competition between infection preventionists and OR managers or directors. The operating room has been that secret area behind the double doors.”

Michael Millenson: “When you dig a little deeper, you end up though with some questions. We’re a big country, and this is an enormous crisis. Well, $180 million? You can barely buy a couple of US senators with that.”

Fibi Attia, MD, MPH, CIC: “There is a daily meeting where we talk about the possibility of getting those COVID vaccines and where are we going to store them. How are we going to distribute them? How many doses do we need? Those kinds of things are being discussed on a daily basis.”

Susan R. Bailey, MD: “Vaccine hesitancy was a huge problem before the pandemic began and has certainly not gotten better since we’ve had COVID and now are looking forward to a COVID-19 vaccine.”

Linda Spaulding: “Infection preventionists, put your tennis shoes on because over the next two months, we’re predicting to see a huge increase.... We have all the holidays coming up. You’re going to have cases from those. Hospitals have to be prepared.”

Ashish Diwanji: “The personal protective equipment made and sold in the US has to abide by the standards set up by NIOSH …. The PPE made and sold from China do adhere to the Chinese standards, but their standards are different than ours.”

Kevin Kavanagh, MD: “Infection preventionists will need to make sure that they still have access to adequate PPE, even if the vaccine comes out [and they] really need to look at the experimental group that was used for the EUA.”

Michael Bell, MD: “The challenge that infection control professionals face has grown tremendously. We’re asking these individuals to not only be experts, but also to take responsibility for such a wide range of activities ... and finding ways to help them accomplish what they’re doing across the whole population of healthcare personnel is the rationale behind Project Firstline.”
